Common Marathon Running Injuries: Sprains/Strains, Tendonitis, Low Back Pain, Iliotibial Friction Syndrome, Plantar Fasciitis, Delayed Onset Muscle Soreness (#NYCmarathon)
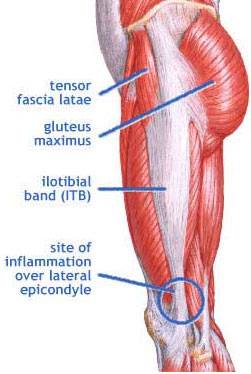
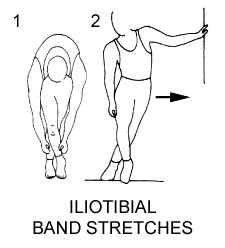
Congratulations again to all of the marathon runners and an even bigger congratulation to those we helped prepare for the run. We are currently treating many runners who sustained overuse injuries during the marathon. Marathon running is such a great sport but can be a cause of low back, pelvic, hip, knee, shin, and ankle/foot pain. When the biomechanics of the shock absorbing joints are compromised or if there is a pre-existing injury and the system is overly challenged- injury, inflammation, and pain can result. Some of the more common running injuries include sacroiliac joint dysfunction, iliotibial (ITB) friction syndrome, shin splints, Achilles tendonitis, and plantar fasciitis. Others may have general low back pain, knee and/or foot pain due to muscle strains and ligamentous sprains. General muscle soreness from running a marathon may not occur until 24-72 hours after the actual race due to Delayed Onset of Muscle Soreness referred to as DOMS. Symptoms can range from muscle tenderness to severe debilitation. Proposed mechanisms of DOMS include lactic acid build-up, muscle spasm, connective tissue damage, inflammation, and enzyme efflux issues. Increased hydration, rest, icing and/or warm baths, electrolyte rebalancing, and soft tissue mobilization/massage from a skilled physical therapist is needed. Other modalities useful in muscle pain include therapeutic ultrasound, electrical stimulation, cold laser, and prescriptive stretching- and we have all of these state-of-the-art modalities at our practice. Overall, physical therapy for marathon-related common orthopedic problems is highly recommended to put you on your road to recovery and fast. When undergoing physical therapy it is important to make sure that there is proper alignment of the facet joints in the lumbar spine and that the pelvic girdle, including the sacroiliac joints, are also properly aligned. Realignment of the pelvis joints is the first intervention in treating all running injuries, especially low back pain and iliotibial friction syndrome. In fact, we saw more iliotibial friction syndrome than any other running injury this year. The incidence is reported to be as high as 12% of all running-related overuse injuries. ITB friction syndrome occurs when there is an imbalance around the pelvis, hip, and knee and upon heel strike during running the ITB becomes aberrantly tensioned and frictions along the lateral femoral epidcondyle. Downhill running especially can predispose the runner to ITB friction syndrome because the knee flexion angle at heelstrike is reduced. In addition, cadaver studies have shown that there is great variation of the widths of IT bands which may predispose a person to injuries. Pain along the ITB or lateral thigh and outside of the knee occurs with ITB friction syndrome. The pain worsens upon increased running. It’s important for the physical therapy to include manual therapies to release tension in the tensor fascia latae muscle (upper attachment site of the ITB), ITB, iliopsoas, quadriceps, gluteus maximus and medius, and lateral hamstrings. Since weakness of the gluteus medius and pelvic floor muscles are common findings with ITB friction syndrome, we prescribe specific exercises to improve their motor recruitment and correct the contraction pattern during the gait cycle and running. The gluteus medius must “turn on” efficiently and strongly during unilateral stance or when one leg is bearing all of the body weight during running otherwise the ITB may compensate. Cross friction massage, ice massage, corrective patella (knee cap) and fibula mobility techniques, foam rolling, therapeutic ultrasound, cold laser, and stretching are other key elements of a rehab program. More info to come about Achilles tendonitis, plantar fasciitis, and shin splints! Keep following our posts!